
Case:
Mrs. K is a 75-year old woman who complains of a painful left knee.
Mrs. K’s symptoms started after she stepped down from a bus with unusual force. The pain became intolerable within about 6 hours of onset and has been present for 3 days now. She otherwise feels well. She reports no fevers, chills, dietary changes, or sick contacts.
On physical exam she is in obvious pain, limping into the exam room on a cane. Her vital signs are temperature, 37.0°C; RR, 12 breaths per minute; BP, 110/70 mm Hg; pulse, 80 bpm. The only abnormality on exam is the right knee. It is red, warm to the touch, and tender to palpation. The range of motion is limited to only about 20 degrees.
Mrs. K has never had a similar episode before. Her other medical problems include diabetes mellitus with diabetic nephropathy, hypertension, and hypercholesterolemia. Her medications are insulin, enalapril, atorvastatin, and hydrochlorothiazide. There is no history of alcohol or drug abuse. Radiographs of the knee demonstrate evidence of mind OA but no evidence of fracture. Joint fluid is aspirated from the patient’s knee.
Mrs. K’s synovial fluid aspiration yielded 25 mL of translucent, yellow fluid. The WBC was about 55,000/mcL with 56% PMNs. The Gram stain was negative, and crystal exam with polarized light microscopy demonstrates negatively birefringent crystals consistent with monosodium urate crystals, thus making the diagnosis of gout.
S: 75 y/o female c/o painful left knee s/p stepping down from a bus with unusual force 3 days ago, w/ increased pain within 6 hours of onset. Medical h/o DM w/ diabetic nephropathy, HTN, hypercholesterolemia. Medications include insulin, enalapril, atorvastatin, and hydrochlorothiazide. She denies fevers, chills, dietary changes, sick contacts, h/o alcohol/drug use, similar episode in the past.
O: Temperature, 37.0°C; RR, 12 breaths per minute; BP, 110/70 mm Hg; pulse, 80 bpm
Lower Extremity: right knee is warm to the touch, tender to palpation, ROM 20 degrees, radiographs shows mild OA, no fx.
A: 75 y/o female w/ right knee tenderness and limited ROM w/ mild OA, R/O gout.
P: Gram stain and crystal exam w/ polarized light.
Summary:
Patients with joint pain require a detailed history and physical exam, sometimes followed by sampling of joint fluid and analyzing radiologic and serologic tests. The patient’s exam revealed inflammation of the joint with limited ROM, signifying that articular structures are affected and limiting the differential diagnosis to septic arthritis, pseudogout and gout. Gout is considered more than others due to patient’s age, single inflamed joint and it’s high prevalence. The fact that patient has maximal inflammation for less than a day, monoarthritis, asymmetric joint swelling and joint erythema points it ever more toward gout, but it is still not certain due to patient’s history of hypertension and use of thiazide. Some other alternative diagnoses to consider are Calcium Pyrophosphate Deposition Disease (CPPD), Septic Arthritis, Disseminated Gonorrhea and Lyme Disease. CPPD presents in older patients, with either an acute flare or degenerative arthritis with radiograph ruling out Osteoarthritis. Septic arthritis presents as subacute joint pain, low-grade fever and worsening pain/disability. Disseminated Gonorrhea presents with severe pain to wrists/hands/knees and fever in young/sexually active women. Lyme Disease presents with acute knee pain usually in the area where the disease is widespread. In this particular case, acute gout is considered due to patient’s inflamed joint and high WBC counts. The positive crystal exam makes the diagnosis of gout possible. Next course of action would be to treat the patient with NSAIDs and colchicine. Prophylactic therapy is not necessary due to it being the patient’s first attack.
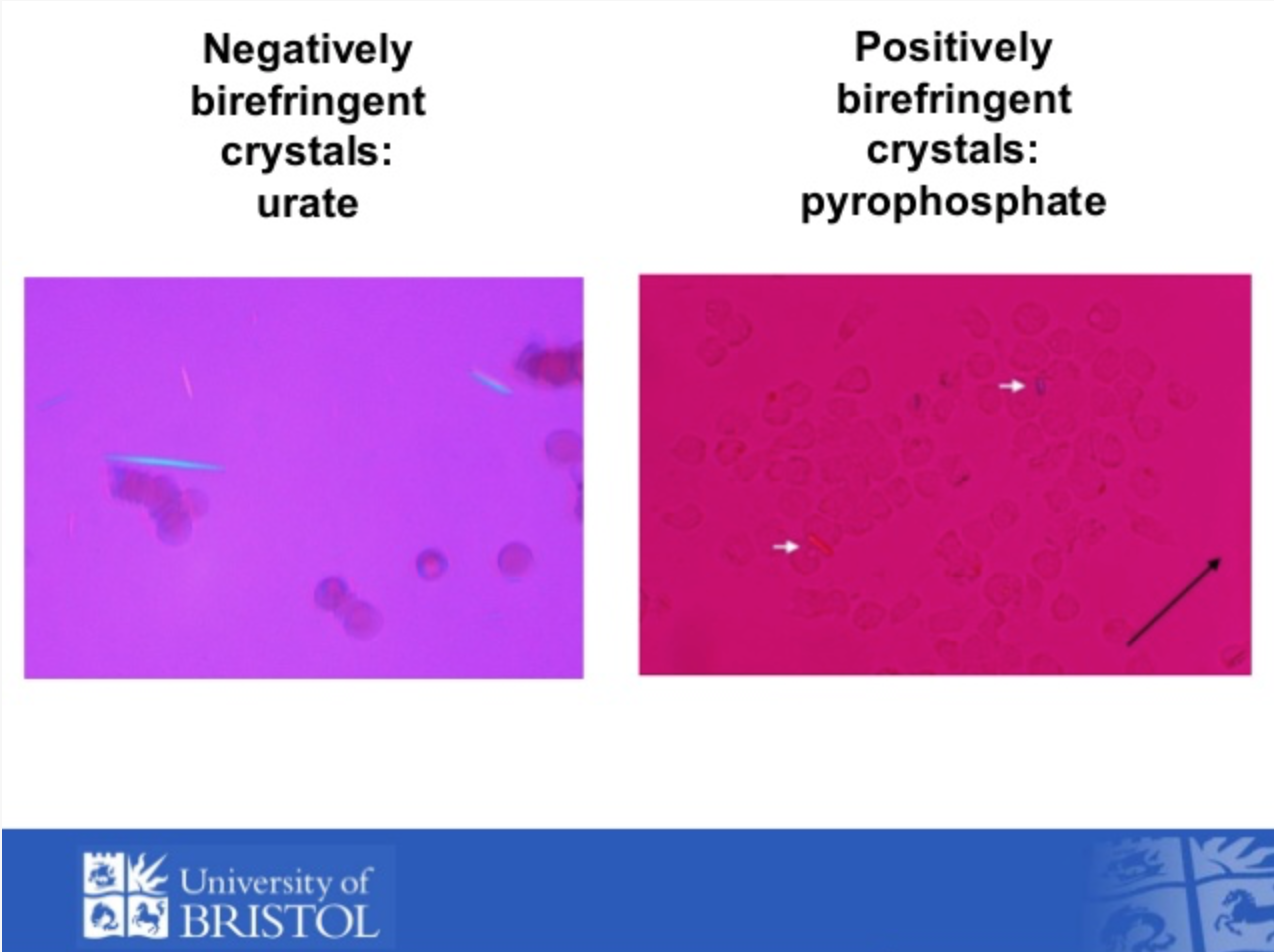
Polarized light microscopy
Reflection:
Prior to this exercise, I had no experience writing SOAP notes. I understood the general process, but the fact that the patient in my case already had a diagnosis threw me off. From my understanding, in my SOAP note I had to arrive at a diagnosis, which is what I attempted to do. Additionally, I did not know that the Plan portion has to include a plan for all current medical problems, which I learned while doing a SOAP note for another course. Overall, I found the exercise to be an informative experience. I believe with practice I will get better at writing SOAP notes, which will be beneficial in my future career.

This entry is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International license.